Hereditary Hemorrhagic Telangiectasia (HHT)
Hereditary Hemorrhagic Telangiectasia (HHT) is a genetic disorder of the blood vessels which affects approximately one in 5,000 people. The disorder is also referred to as Osler-Weber-Rendu Syndrome. HHT is caused by a mutation in one of several HHT-associated genes. HHT is autosomal dominant, which means that if one of your parents or a sibling has HHT, there is a 1 in 2 chance (50%) that you will have HHT.
The HHT Center of Excellence at UCSF is the only location in Northern California that specializes in the diagnosis and treatment of this disorder.






Common Problems:
Pulmonary Arteriovenous Malformations (PAVMs)
Approximately 40 percent of people with HHT have arteriovenous malformations in the lungs (pulmonary AVM or PAVM). People with HHT 1 (ENG) are five to ten times more likely to have PAVMs than those with HHT 2 (ACVRL1). PAVMs, particularly during pregnancy, have a risk of rupturing when blood volume tends to increase. This can be life-threatening. However, there are additional concerns about untreated PAVMs.
Normally, the lung arteries get smaller and smaller as they go deeper into the lungs, similar to the branches of a tree. At the ends of these artery branches, hair-like blood vessels called capillaries join the arteries and veins. These capillaries perform many important functions including allowing passage of oxygen into the blood as well as filtering the blood of impurities (clots, bacteria, air bubbles) before the blood circulates to the brain. With a PAVM, these capillaries are missing, and the artery connects directly to the vein. If the artery leading to the PAVM is larger than two to three millimeters in diameter, small blood clots can travel through the PAVM and go into the brain, causing a stroke. Bacteria can also travel through PAVMs and result in brain abscesses (a brain infection). Stroke and brain abscess can be life-threatening. Fortunately, PAVMs are almost always treatable with a procedure called pulmonary artery embolization. Learn more (pdf)
Screening
An echocardiogram with bubble study is the recommended test of choice for PAVM screening. This test uses ultrasound (sound waves) to determine if injected saline bubbles can get through the lung circulation and be seen back in the heart.
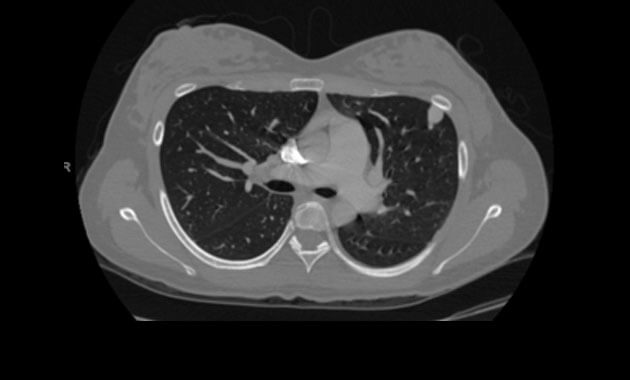
A chest CT scan may also be performed to evaluate for PAVMs. It is also highly sensitive for detection of pulmonary AVMs, but it involves radiation exposure. For this reason, a chest CT is usually reserved for those patients with known PAVMs or a positive echocardiogram with bubble study to determine if treatment is necessary and to determine the anatomy of the AVM and treatment options.
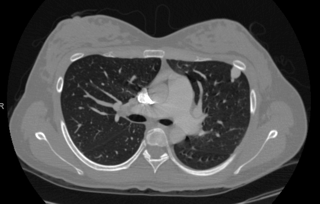
Chest CT depicting
Pulmonary Arteriovenous Malformations (PAVMs).
Treatment
A pulmonary angiogram and embolization is a minimally-invasive procedure performed by an interventional radiologist in an angiography suite. The patient is given sedation for this procedure. A catheter (a small tube) is inserted into an artery in the top of the thigh and directed through the body to the site where the embolization will be performed. An embolization coil is then injected through the catheter to block the blood flow through the AVM. After the procedure, the patient is transferred to the recovery area, where he or she is observed for several hours before being discharged home.

Pulmonary angiogram depicting
Pulmonary Arteriovenous Malformations (PAVMs).
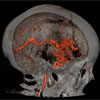
Brain Arteriovenous Malformations (AVMs)
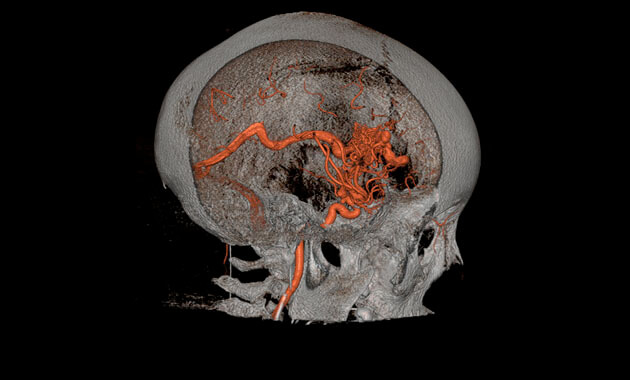
Brain (or cerebral) AVMs are found in about five to twenty percent of people with HHT and can also be successfully treated in most cases. They can be life-threatening or disabling if they bleed. Since they often do not cause warning symptoms prior to bleeding, we recommend screening for them in all people with HHT, even infants. Other types of brain vascular malformations, such as capillary telangiectasias, cavernous malformations, and venous malformations, may be seen in HHT patients. It is not clear if these malformations are seen any more commonly in HHT patients than in patients without HHT, but they are less risky than AVMs and often do not require treatment. Learn more (pdf)
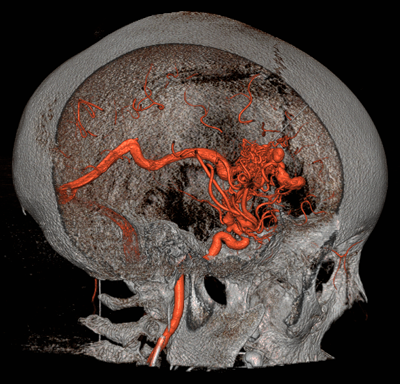
Brain Arteriovenous Malformations (AVMs).
Screening
Magnetic resonance imaging (MRI) of the brain is the recommended test for identifying cerebral AVMs. It utilizes strong magnetic fields to form images of the body. No radiation is used during this study. The duration of the procedure will vary, but the average is 60 minutes. The patient is required to lie still during the actual MR scanning. If the patient has claustrophobia, the doctor may prescribe an oral medication to bring along for the MRI appointment.
A cerebral angiogram is a minimally-invasive procedure performed by a neurointerventional radiologist in an angiography suite. The patient is given general anesthesia or conscious sedation for this procedure. A catheter (a small tube) is inserted into an artery in the top of the thigh and directed through the blood vessels in the body to arteries in the neck or the brain. The patient may require treatment, called an embolization, at the time of the procedure. After the diagnostic cerebral angiogram, if there is no embolization involved, the patient is transferred to a recovery area, where he or she is observed for several hours before being discharged home.
Treatment
A cerebral embolization is a minimally-invasive procedure performed by a neurointerventional radiologist in an angiography suite. The patient is given a general anesthesia for this procedure. A catheter (a small tube) is inserted into an artery in the top of the thigh and directed through the blood vessels of the body to the arteries in the neck or the brain. An embolization material is then injected through the catheter to treat the AVMs. This material could be small flexible coils, small plastic beads, or medical glues. After the procedure, the patient is transferred to the intensive care unit, where he or she is observed overnight before being discharged home unless the patient is then scheduled for additional surgery.
Gamma Knife treatment is a type of focused radiation that destroys the AVM tissue. This is sometimes done in lieu of or after embolization to ensure that the AVM is cured.
Liver Arteriovenous Malformations (AVMs)
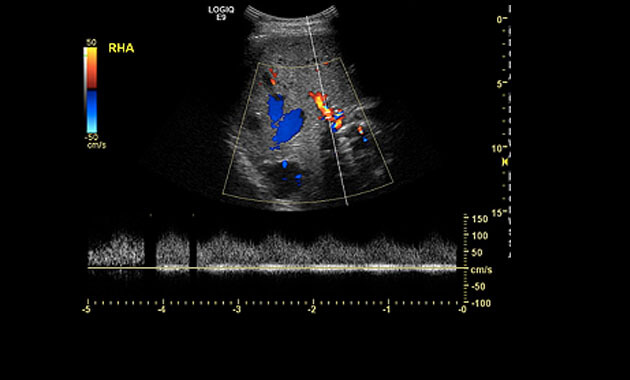
Liver AVMs are found in 32 to 74 percent of people with HHT, but they only cause symptoms in an estimated eight percent. AVMs in the liver occasionally cause heart failure, usually later in life. Heart failure can occur if the heart has been overworked for years, pumping extra blood through the low resistance pathway of a liver AVM (shunt), as well as through all the normal vessels of the body. There are several other even more rare and complex complications that can result when HHT affects the liver. Few physicians outside of clinics that specialize in HHT are familiar with these complications. Learn more (pdf)
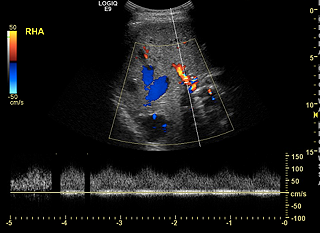
Ultrasound depicting a
Liver Arteriovenous Malformation (AVM).
Screening
A liver ultrasound uses reflected sound waves to produce a picture of the organs in the abdomen. No radiation is used during this study, and it is therefore the preferred method for screening liver AVMs.
An abdominal CT or MRI scan may also be performed to evaluate for liver AVMs.
Treatment
Liver AVMs rarely cause complications, and treatment is not recommended. Liver biopsies should also be avoided due to the risk of bleeding. Liver AVMs can result in elevated liver enzymes, which are usually not clinically significant. In rare cases, large or diffuse liver AVMs can result in heart failure. Those patients with significant liver AVMs should be followed routinely by a cardiologist.
HTT Center of Excellence Team
Because HHT symptoms can affect various parts of the body often early in a patient’s life, our team of specialists at the UCSF HHT Center of Excellence consists of experts in the fields of Interventional and Neurointerventional Radiology, Pediatrics, Medical Genetics, Hematology, Otolaryngology/Head and Neck Surgery, Cardiology, Gastroenterology, Neurology and Pulmonology.
HHT Center of Excellence Co-Directors


The UCSF HHT Center of Excellence
Interventional Radiology Scheduling
(415) 353-8867

UCSF Imaging Center at China Basin
185 Berry Street, Suite 180, Lobby 6
San Francisco CA 94107
(Free validation for parking at this location)
Pediatric Patients
UCSF Ron Conway Family Gateway Medical Building,
5th Floor, Reception area 5A
UCSF Medical Center at Mission Bay
1825 Fourth Street
San Francisco, CA 94158
Patient Care Coordinator
Torianna Lomax
Phone: (415) 353-8867
Fax: (415) 353-4503
Email: [email protected]
Clinical Coordinator
Daniel Langston, NP
Ph: (415) 353-4872
Fx: (415) 353-4503
Email: [email protected]