
Hives (Urticaria)
Mild (scattered and/or transient)
| Treatment | Dosing |
| No treament often needed; however, if sympotmatic, can consider: | |
| Diphenhydramine (Benadryl®)* | 25-50mg PO |
| or | |
| Fexofenadine (Allegra®)** | 180mg PO |
Moderate (more numerous/bothersome)
| Treatment | Dosing |
| Monitor vitals | |
| Preserve IV access | 25-50mg PO |
| Consider diphenhydramine (Benadryl®)* | |
| or | |
| Fexofenadine (Allegra®)** | 180mg PO |
| or | |
| Consider diphenhydramine (Benadryl)* | 25-50mg IM or IV (administer IV dose slowly over 1-2 min) |
Severe (widespread and /or progressive)
| Treatment | Dosing |
| Monitor vitals | |
| Preserve IV access | |
| Consider Diphenhydramine (Benadryl®)* | 25-50mg IM or IV (administer IV dose slowly over 1-2 min) |
*Note: all forms can cause drowsiness; IM/IV form may cause or worsen hypotension.
**Note: second generation antihistamines cause less drowsiness; may be beneficial for patients who need at to drive themselves home.
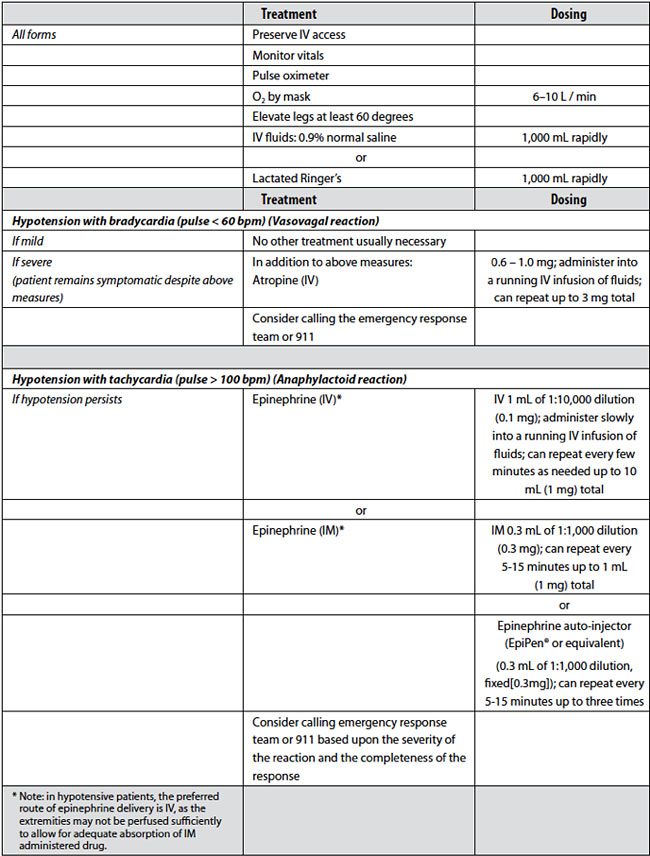
Diffuse Erythema
All forms
| Treatment | Dosing |
| Preserve IV access | |
| Monitor vitals | |
| Pulse oximeter | |
| O2 by mask | 6-10 L/min |
Normotensive
| No other treatment usually neeeded. |
Hypotensive
| Treatment | Dosing | |
| IV fluids 0.9% normal saline | 1,000 mL rapidly | |
| or | ||
| Lactated Ringer's | 1,000 mL rapidly | |
| If profound or unresponsive to fluids alone, can also consider |
Epinephrine (IV)* | IV 1 mL of 1:10,000 dilution (0.1mg); administer slowly into a running IV infusion of fluids; can repeat every few minutes as needed up to 10 mL (1mg) total |
| or (if no IV access available) | ||
| Epinephrine (IV)* | IM 0.3 mL of 1:1,000 dilution (0.3mg): can repeat every 5-15 minutes up to 1 mL (1mg) total |
|
| or | ||
| Epinephrine auto-injector (EpiPen or equivalent) (0.3 mL of 1:1,000 dilution, fixed ([0.3mg]); can repeat every 5-15 minutes up to three times |
||
| Consider calling emergency response team of 911 |
*Note: in hypotensive patients, the preferred route of epinephrine delivery is IV, as the extremities may not be perfused sufficiently to allow for adequate absorption of IM administered drug.
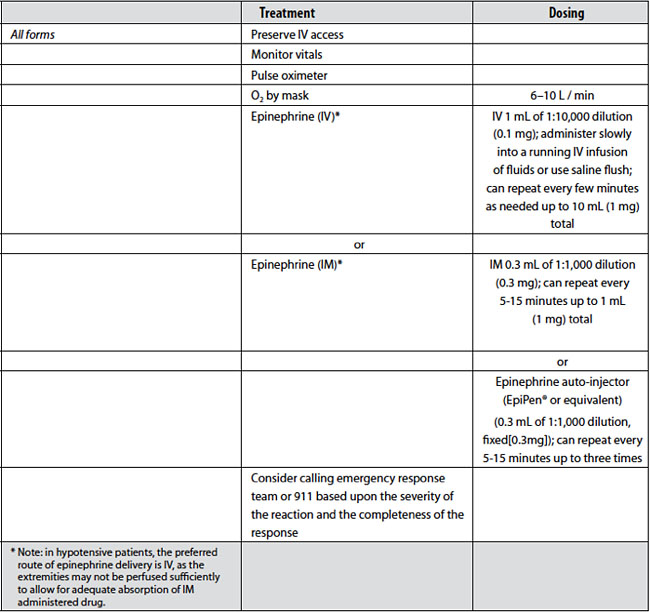
Bronchospasm
All forms
| Treatment | Dosing |
| Preserve IV access | |
| Monitor vitals | |
| Pulse oximeter | |
| O2 by mask | 6-10 L/min |
Mild
| Treatment | Dosing |
| Beta agonist inhaler (Albuterol) | 2 puffs (90 mcg/puff) for a total of 180 mcg; can repeat up to 3 times |
| Consider sending patient to the Emergency Department or calling emergency response or 911, based upon the completemness of the response to the beta agonist inhaler |
Moderate
| Treatment | Dosing |
| Beta agonist inhaler (Albuterol) | 2 puffs (90 mcg/puff) for a total of 180 mcg; can repeat up to 3 times |
| Consider adding epinephrine (IM)* | IM 0.3 mL of 1:1,000 dilution (0.3mg): can repeat every 5-15 minutes up to 1 mL (1mg) total |
| or | |
| Epinephrine (IV)* | IV 1 mL of 1:10,000 dilution (0.1mg); administer slowly into a running IV infusion of fluids or use saline flush; can repeat every few minutes as needed up to 10 mL (1mg) total |
| Consider calling emergency response team or 911 based upon the completeness of the response |
Severe
| Treatment | Dosing |
| Epinephrine (IV)* | IV 1 mL of 1:10,000 dilution (0.1mg); administer slowly into a running IV infusion of fluids or slow IV push followed by a slow saline flush; can repeat every few minutes as needed up to 10 mL (1mg) total |
| or | |
| Epinephrine (IV)* | IM 0.3 mL of 1:1,000 dilution (0.3mg): can repeat every 5-15 minutes up to 1 mL (1mg) total |
| or | |
| Epinephrine auto-injector (EpiPen or equivalent) (0.3 mL of 1:1,000 dilution, fixed ([0.3mg]); can repeat every 5-15 minutes up to three times |
|
|
AND Beta agonist inhaler (Albuterol) |
2 puffs (90 mcg/puff) for a total of 180 mcg; can repeat up to 3 times |
| Calling emergency response team of 911 |
*Note: in hypotensive patients, the preferred route of epinephrine delivery is IV, as the extremities may not be perfused sufficiently to allow for adequate absorption of IM administered drug.
Laryngeal Edema
Hypotension (systolic blood pressure < 90mm Hg)
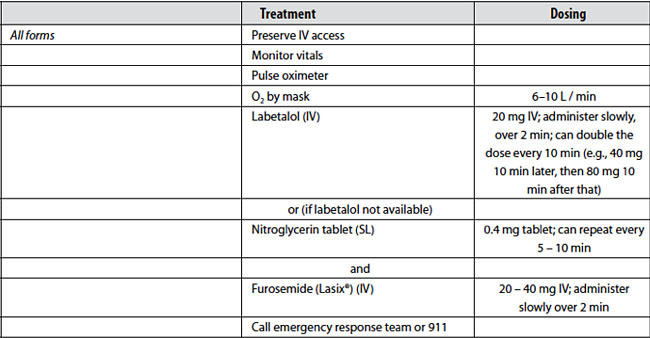
Hypertensive Crisis
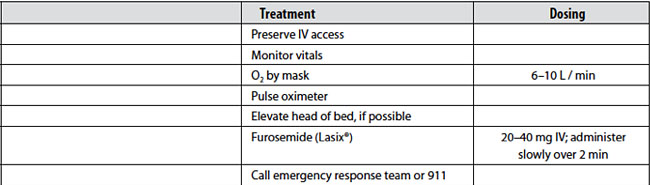
Pulmonary Edema
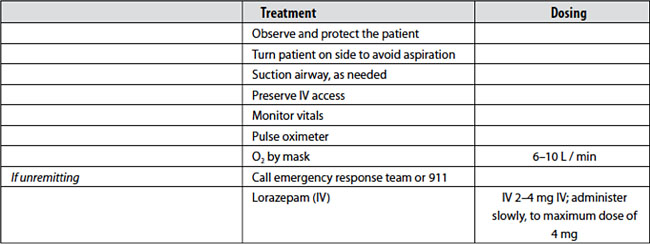
Seizures/Convulsions
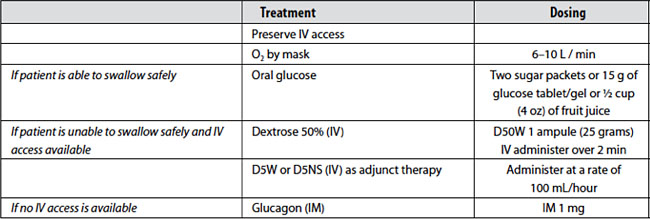
Hypoglycemia
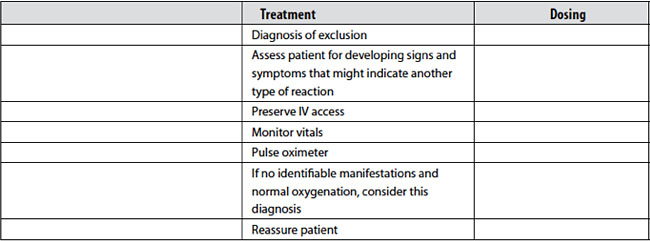
Anxiety (Panic Attack)
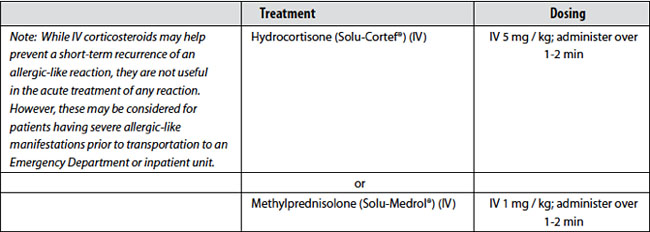
Reaction Rebound Prevention
Last updated: 28 August 2015