
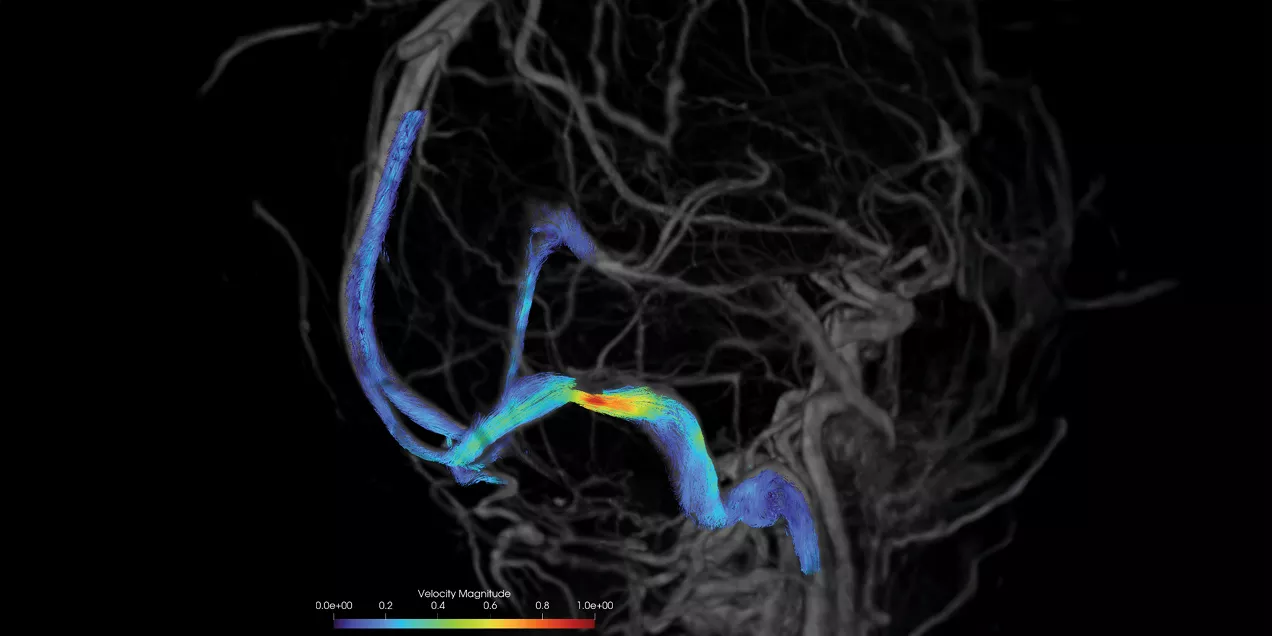
Velocity Magnitude in Venous Sinus Stenosis Using 4D Flow MRI
Imaging Pulsatile Tinnitus with 4D Flow MRI
Patients with pulsatile tinnitus are beset by a sound that surges with every beat of their heart. For those who seek medical intervention, the noise is often so loud it interferes with their hearing and sleep. This rare but debilitating condition can cause anxiety, depression, and chronic fatigue. While surgical treatment is possible, the mechanics of how and why these sounds arise are poorly understood.
Postdoctoral scholar Jonas Schollenberger, PhD, works with David Saloner, PhD, to understand the physics of pulsatile tinnitus and develop MRI sequences capable of non-invasively imaging these and other blood flow problems in the brain. A catheter-based angiogram is the current diagnostic standard to identify vascular abnormalities generating such sound. However, this invasive procedure is mostly limited to qualitative assessment of anatomical features such as the presence of stenosis.

We know pulsatile tinnitus is related to blood flow, because it syncs to the heart, but we don’t fully understand what specific hemodynamic features cause it.
Seeking to expand our understanding of pulsatile tinnitus, Schollenberger uses 4D Flow MRI to non-invasively image blood flow within arteries to gather complementary quantitative data on blood velocity, turbulent kinetic energy, and pressure gradients. These MRI images show the areas of turbulent blood flow that may cause the characteristic sound of pulsatile tinnitus.

Normally, your blood flows in a smooth, or laminar, pattern, even with the pulses of your heartbeat. However, certain malformations such as stenosis that constrict artery walls can accelerate the blood as it squeezes through the narrowed passage. When the narrowed section opens up, a “jet” of blood dissipates into a chaotic turbulent area like rapids in a river. If that turbulence occurs within a few inches of your ear, that may produce a noticeable sound.
Schollenberger validates the 4D flow imaging sequence through trials on idealized models, or phantoms, a key step towards carrying this new technique to the patient. These simplified rigs pump liquid through a constriction so he can validate the MRI acquisition sequences in stable and consistent trials. Collaboration with the UCSF Pulsatile Tinnitus Clinic, led by Mathew Amans, MD, allows Schollenberger and Saloner access to the information they need to know their simulation conditions match the real-world requirements.
The new wealth of data that 4D Flow MRI provides can allow researchers and clinicians to move away from purely anatomical to hemodynamic-based quantitative metrics and better understand the mechanisms of pulsatile tinnitus and better stratify the risk of any treatment procedures. Schollenberger hopes that his work will reduce the necessity of catheter-based angiography by providing an alternative, non-invasive approach to assess this condition.